|
There may be occasions when you’ll want to revisit a past session to either retreat the patient/client for that category or to treat for items you didn’t treat before but wish you had. This might occur when you realized you didn’t set the Range low enough.
For example: you realized you accepted the software’s range suggestion then later realized it was 55 instead of 10, and you want to follow my advise to never have a Range less than 10. You might want to correct this mistake. You do NOT want to run the BioSurvey again so this is how you do it:
You should rarely have to resort to this procedure, but now you know how to do it (if you didn’t already know).
0 Comments
I received a call from a practitioner a few weeks ago about reactions a couple of her patients had some time after receiving a SET-DB™ treatment. Both patients were children, siblings, about the same age. As I recall, one broke out with hives about four hours after a treatment for amino acids, the other about four days after the same treatment. The parent claims neither were given a protein meal during the four-hour avoidance period.
So, what gives? First, after performing thousands of SET-DB™ treatments, no patient of mine ever reported a negative reaction after a treatment, other than what I write about in the Practitioner’s Manual. If the treatment was performed correctly and the patient observed the avoidance period, the only negative reactions ever reported to me were fatigue and a dull headache (from the New-Stim). That’s not to say a negative reaction to a treatment could never happen, but the odds are right up there with winning the Powerball—not real likely. So, again, what gives? The obvious answer is they reacted to something they weren’t treated for, which could be just about anything as they’d only had one treatment. To put a finer point on it, it’s likely they reacted to something new in their shared environment. New allergen — new symptom. Here’s what I would’ve done if this had happened to me:
To sum up, as a general rule it’s always better to try to get the patient to go through the treatment program you think they need. This should be the inhalants program or the food and nutrient program, or both. Anything less is doing the patient a disservice by allowing them to leave your care with sensitivities, which will over time contribute to poor health. (Small children can be an exception.) Also, properly educate your patients/clients BEFORE they come to see you. This not only saves you time on the first visit, a better-educated patient is a better patient, and better patients will understand they need to get all their sensitivities corrected. This was a fibromyalgia patient of mine from 2007. There's nothing "special" to be learned from this case. I only present it to once again demonstrate how quickly fibromyalgia patients can be feeling better with the SET-DB™ Fibromyalgia Treatment Program, and to lead into a discussion of why I sold the program as a series of treatments instead of allowing patients to pay visit-by-visit. One thing different about this 41-year-old single mother was, she was still able to work full time. She had 2 or 3 kids (remember, this was 10 years ago) and lived with her mother. Speaking of her mother, as I recall she was so happy with her daughter's recovery that she offered to write a testimonial as well. Here are the 2 testimonials:  Notice how the patient wrote "I wanted to die." It was obvious she wasn't suicidal, but felt she had very little quality of life. Yes, she was able to work full time, but you and I know that some people can push through pain better than others. And her job was the main source of for the household. Here's her Symptom Intensity Graph:  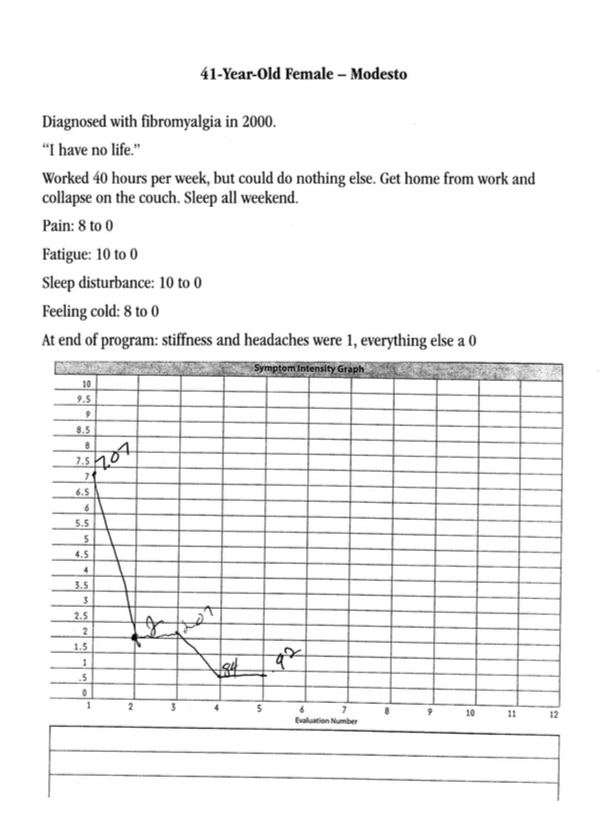 We see here the typical free-fall in the graph from when the patient presented to when they completed their first symptom questionnaire, after their first 6 visits. She went from 7.07 to 2, nearly a 75% drop in her overall symptom pattern (I tracked the top 13 symptoms of fibromyalgia). She ended at .92, an 87% drop in her overall symptom profile.
Now, what might have happened if I didn't sell the treatment program as a package and the patient was paying visit-by-visit? She likely would have dropped out after 6 treatments, or earlier. I can see where some may argue in favor of her stopping the program early. After all, at 6 treatments in her symptoms had dropped 75%. (The FDA approved Lyrica for the treatment of fibromyalgia after a couple of trials where it dropped ONE symptom—pain—by about half that.) It comes down to your treatment philosophy: how well do you want your patients to get? I wanted to help my patients get as well as possible. If you learn one thing from reading Dr. Nambudripad's first book, Say Goodbye to Illness, it should have been ANY sensitivity can cause ANY symptom. I wanted to get rid of as many of my patients' sensitivities as they'd let me. Overall, the people who went through the SET-DB™ Fibromyalgia Treatment Program saw, on average, their symptom profile drop by 67% and 80% of the cases were successful, meaning both the patient and me were happy with their outcome. A couple of days ago I gave my wife a new supplement, standardized black cohosh, to see if it would help minimize (or eliminate) the few hot flashes she's been getting. I had her take her supplements in the morning, then we went out to do some shopping.
About two hours later, while scratching her arm, she asked me if I gave her anything new. I said yes and told what it was, and why. She replied that she's been itching like crazy for about an hour and asked if she could be allergic to the new supplement. Of course the answer is "yes." In fact, I should have known better. We've known each other for 20 years and over that time span she's had definite and clear reactions to supplements I've given her. So, when we got home, I had her lie on our portable adjusting table, checked her leg length (always short on the right), then put the bottle of suspicious supplements in her hand. Her right leg went almost another half-inch shorter. I performed the treatment, gave her an adjustment since she was on the table, and had her hold the bottle for 15 minutes. The itching actually got worse for about an hour, then suddenly and completely disappeared. What can we learn from this?
Use the marketing materials included in the program and never stop working on expanding this segment of your practice! Dr. Teryl Boothe P.S. Shoot me an email if you have any questions. 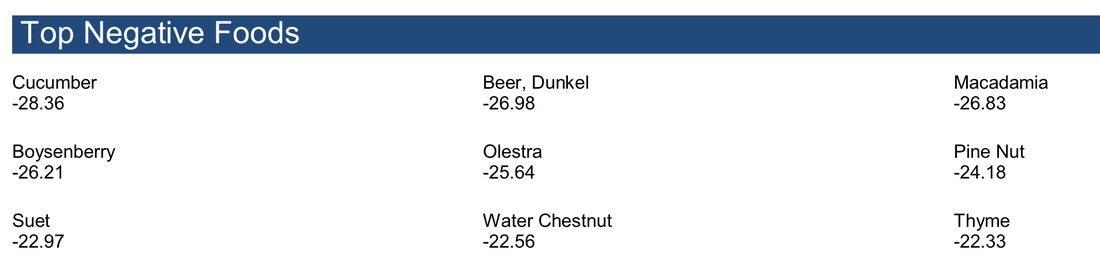 Sample ZYTO Elite report for food testing. I recently had a client who complained about how ZYTO's dR numbers change. For example, if you run a BioSurvey on Monday and again on Tuesday, the dR numbers might be different. Perhaps radically different. The client wondered if he should go back to muscle testing.
Well let's see. A SET-DB office visit shouldn't take longer than five minutes and in that time you could test and treat a patient for literally hundreds of potential sensitivities. How long would that take to muscle test? I'm not going to make excuses for how ZYTO's software operates. dRs are my number one complaint for the ZYTO Elite. Patients, especially men for some reason, obsess over the numbers. "Why is avocado 34 but wheat is 29? I don't notice anything after I eat avocados but I itch after I eat wheat." And on and on. I cover this in detail in my manual and provide scripts and explanations. If you have a ZYTO Elite and am bothered by dRs, here's my advice to you: Let it go. More important than your fussiness about tests being reproducible is helping more patients achieve better health. That's exactly what the ZYTO Elite does. SET-DB treatments work. I saw them work day in and day out for twelve years. I'm so confident they work I quit retesting patients for things they were treated for on their last visit. In my free ten-page report titled What To Do With a ZYTO Elite I explain the simple but powerful procedure I used for years to accentuate SET-DB treatment programs. Patients loved it because it was easy to understand, the treatment was easy to take, and it didn't cost them a lot of time or money. Best of all, it was effective. However it does it, and however goofy those dR numbers may seem, the ZYTO Elite can help you get far more people feeling better faster than anything else I know of. So don't fuss over those dR numbers. Like pretty much everyone in the world, I was skeptical when I first heard that allergies could be fixed. Everyone knows that's not possible, right? That's why I used to joke with my allergy-suffering patients (before I knew better) that if I had a cure for allergies there'd be a line out my door and halfway down the street. They'd smile as best they could and agree.
It was humorous because we knew it wasn't true. Then I found out it was true. I first tried the treatment on my family, of course, then the patient who asked me to learn how to do the treatment. Once I saw that it worked, I was ready to market the treatment. Shortly after I bought a BioMeridian MSAS-Pro, I had a patient referred in by a family member. My family, that is. Her problem was, she had anaphylactic reactions to pretty much all fruit. The only way she could eat fruit was if it was boiled to mush (why she would even want to eat boiled-to-mush fruit is a question I never asked her). As I teach in SET-DB, I required her to go through the nutrient groups before we started treating foods, in her case, fruit. Because I didn't know better, I treated the category called "phenolics" fifth or six (it was a long time ago). I recall she came in on a Monday and got a treatment every day that week (so it was treated fifth). Friday was phenolics. She returned on Monday and told me she ate a whole bag of oranges over the weekend. (I did NOT tell her to do that nor did I suggest she try eating oranges.) THAT was a miracle to me, and certainly to my patient. It's likely that treating her for the phenolic gallic acid did the trick. After that I witnessed many "miracles" in my practice. I came to call the treatments for amino acids and phenolics (two separate treatments) my "miracle treatments" because many patients had seemingly miraculous results after one of them. This is why they're treated first and second in SET-DB. |
AuthorDr. Teryl Boothe and selected guests. Archives
January 2024
Categories
All
|
 RSS Feed
RSS Feed